Bio‑Resilience Engine
We require a multi‑layer architecture, i.e., a macro level (Geo‑Resilience), a meso level (Compass sectors), and a micro level (e.g., the Winter PK Matrix), because the Compass addresses not only governance but also bio‑governance.
The Bio‑Resilience Engine constitutes the physiological deep structure of the Geo‑Resilience Compass: it illuminates how environmental stressors, seasonal dynamics, infectious pressures, and pollutant exposures penetrate the human body and recalibrate immune axes, barrier integrity, microbiome composition, and pharmacokinetic behavior. What appears in the Compass as strategic orientation finds its biological foundation here. The Bio‑Resilience Engine demonstrates that resilience is not merely a matter of governance, infrastructure, or data, but a living interplay between environment, biology, and context. It links, for example, the Winter‑PK‑Matrix I developed with the spatial and systemic dimensions of the Geo‑Resilience Framework, opening an expanded plane of understanding: resilience becomes not only navigable, but biologically measurable, anticipatory and actively shapeable.
The Bio‑Resilience Engine forms a kind of biological deep layer of the Geo‑Resilience Center and is intended to reveal how environment, climate, infections, pollutants, and pharmacokinetics shape (or could shape) the operational resilience of societies.
I developed the PK‑Winter Matrix, together with the 17/8 model, to render the notion of “winter” globally interoperable — beyond temperature, climate, and meteorological convention. In many parts of the world, winter does not signify cold, but seasonal immune shifts, altered barrier functions, infection pressure, environmental stress, and pharmacokinetic modulation. The PK‑Winter Matrix is designed to translate these biological patterns into a universal model capable of functioning across both temperate and tropical climates. It establishes a shared language for seasonal resilience mechanisms and enables winter to be understood as a global biological dynamic — independent of how it manifests climatically.
In this context, I would like to refer to winter as a global biological archetype, as it reveals biological patterns across the world. When I define “winter” biologically here, I do not mean cold, snow, or seasons, but a recurring physiological pattern that can occur anywhere on the planet – even in the tropics.
Biologically, winter means for me:
• less UV light → Vitamin D axes change
• more indoor time → higher infection burden
• dry air / barrier stress
• increased pollutant exposure (heating, smog, inversion)
• AHR activation
• seasonal immune shifts (Th17, IL‑6, TBX21)
• altered microbiome profiles
• altered pharmacokinetics (transporters, CYPs, clearance)
So we should ask ourselves how exactly these patterns (i.e., only through different mechanisms) manifest globally:
• Winter ≠ temperature
• Winter = biological dynamics
• Winter is globally interoperable
• Winter is a universal pattern
• Winter is a resilience phenomenon
• Winter is a PK modulator
• Winter is a governance signal
And all of this together forms the logic that underpins the 17/8 model. The 17‑axis (AHR/Th17/TBX21) and the 8‑axis (barrier/infection/microbiome) are universal biological axes that can be seasonally modulated anywhere in the world.
Even in tropical countries there are:
• infection seasons
• smog seasons
• rainy seasons
• dry seasons
• seasonal immune axes
• seasonal PK shifts
→ Winter is a biological pattern, not a weather phenomenon.
The countries selected below are, of course, only examples, and I assembled them for my Winter PK Matrix (immune axes, barrier, microbiome, transporters, PK shifts) based on the following criteria:
- Geo Resilience Compass (environmental change, biological risks, infrastructure, society)
- climate (temperate vs. tropical)
- environmental stress (smog, PM2.5, AHR ligands)
- infection patterns
- demographics & health systems
- technological maturity
- data availability
The order listed here does NOT represent a ranking or evaluation.
Why?
Because these countries simultaneously have:
• strong seasonality or tropical stress
• high environmental burden (AHR axis)
• high infection pressure (8‑axis)
• robust digital infrastructure
• high governance maturity
→ They would all be perfect ecosystems for the Geo Resilience Framework + Winter PK Matrix.
PK-Winter-Matrix

Note: These genes are only a small selection. Of course, COMT, NAT2, EPXH1, MTHFR, CYP2C19, 3A4, 3A5, 2D6, 1A1, 1A2, SOD2, GSTs and many others should also be included here.


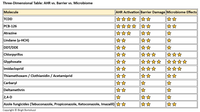
Source/Note: Own creation (December 29, 2025) — The wonderful contributions and the PK Weekly Dose by Prof. Eric Chan (NUS Singapore) on LinkedIn consistently inspire me and encourage me to explore PK and toxicology topics from a 360‑degree perspective. I hold Eric in very high regard, and for this reason, I would like to dedicate this matrix, which I developed, to him.
The 17/8 model illustrates a multi layered system in which the immune axis (17 axis: TBX21 driven Th1/Th17 polarization) and the viral axis (8 axis: Adenovirus and antiviral signaling) interact bidirectionally. These master axes regulate transporter and metabolic nodes (SLC28A3, SLC22, ABC transporters, CMPK1, CYP enzymes), which in turn determine pharmacokinetics, antiviral capacity, and tissue susceptibility. Winter associated pollutants (PM, NOx, AHR ligands, oxidative stress) modulate all layers by activating NRF2, NF κB, and mTOR pathways, thereby shifting immune tone, transporter expression, and viral dynamics. Genes are not isolated markers — they are hubs in a 17/8 system of immune regulation, transport, metabolism, infection, and environment.
The 17 axis (TBX21/Th17) and the 8 axis (adenovirus/infection) are the two master regulators that connect everything together.
1. Japan: Japan exhibits pronounced seasonality, which in winter is associated with clear peaks in respiratory infections, a possible significant decline in vitamin D levels, and plausible seasonal pharmacokinetic shifts. This seasonal dynamic may influence barrier integrity, immune axes, and transporter expression, making Japan an ideal model environment for the Winter PK Matrix. In urban centers such as Tokyo, Osaka, and Nagoya, relevant exposures to PM2.5, NOx, and traffic‑related emissions occur. These environmental factors activate AHR‑dependent signaling pathways and modulate inflammatory, metabolic, and transporter‑specific processes — a central mechanism linking environmental stress to pharmacokinetics. Japan is also among the world’s leading nations in pharmacokinetics, DMPK, transporter research, systems biology, and immunology. The combination of excellent research infrastructure, high data quality, and an increasingly aging population — with elevated barrier vulnerability, immunosenescence, and potentially altered PK profiles — could make Japan a particularly relevant application case for integration into the Geo Resilience Compass.
2. Singapore: Singapore has a tropical climate with consistently high temperatures and humidity throughout the year, which could lead to a potentially constant infection burden and clearly defined seasonal patterns, particularly in the context of respiratory and vector‑borne diseases. In addition, the region is regularly affected by pronounced PM2.5 exposures, intensified by transnational haze events originating from Indonesia. These episodic but intense air‑pollution phases make the AHR‑dependent environmental and inflammatory axes biologically highly relevant and influence barrier integrity, transporter expression, and immunological signaling pathways. At the same time, Singapore is among the global leaders in biomedicine, systems biology, pharmacology, and AHR research. The combination of highly advanced research infrastructure, excellent data availability, and a strongly digitalized healthcare landscape makes Singapore an ideal application case for the Geo Resilience Compass.
3. South Korea: South Korea is a central “hotspot” for environmental–biological interactions, as the country exhibits high fine‑dust exposure, particularly from PM2.5 and the seasonally occurring Yellow Dust events, which consist of desert dust and anthropogenic emissions. These exposures activate AHR‑dependent environmental and inflammatory axes and significantly influence barrier integrity, transporter expression, and immunological signaling pathways. At the same time, South Korea shows pronounced seasonality with clear winter effects, which may be reflected in altered infection patterns, barrier stress, vitamin D modulation, and plausible seasonal PK shifts. The combination of climatic seasonality and high urban exposure makes the country an ideal model environment for the Winter PK Matrix. South Korea is also among the world’s leading nations in pharmacogenetics, transporter research, immunology, and systems biology. The excellent data availability, high technological maturity, and dense urban infrastructure make it an optimal application case for the Geo Resilience Compass. Thus, South Korea could represent a highly relevant environment in which environmental stress, seasonality, immunomodulation, and pharmacokinetic dynamics interact in particularly pronounced ways.
4. Russia: Russia is, from a biological, climatic, and environmental‑health perspective, one of the highly relevant countries where the Winter PK Matrix applies. It represents a winter extreme case, an AHR hotspot, an infection hotspot, a barrier‑stress hotspot, a PK‑shift hotspot, and geographically a vast test field for the PK‑Winter‑Matrix as well as an ideal application case for the Geo Resilience Compass.
- Russia has enormous climatic diversity → the model could potentially function across all zones.
- Russia has high industrial exposure → environmental–biology couplings are strongly pronounced here.
- Russia has vast geographical ranges → ideal for the Geo Resilience Compass.
- Russia has strong seasonal infection patterns → this is where I see the 8‑axis fully active (→ barrier + microbiome + transporters may change → PK shifts thereby become clinically relevant): RSV waves, influenza waves, adenovirus waves, bacterial winter infections, and possible barrier damage due to dry air.
- Russia possesses extreme environmental stressors → this is where I see the AHR/NRF2 axes maximally active, i.e., high industrial emissions, extreme winter smog episodes, high fine‑dust exposure in cities, and strong AHR ligands (wood, coal, industry, heating). Transporters (SLC22, ABCB1) are strongly modulated → PK profiles could therefore also change substantially.
- Russia is among the countries with the strongest winter effects worldwide: long periods of darkness, extreme temperature differences, pronounced winter infection waves; plausibly, strong seasonal immune shifts and possible PK changes due to cold, nutrition, and stress could also occur. From the perspective of the Winter PK Matrix, Russia would be a potential hotspot, and the matrix could provide valuable insights here.
5. Ukraine: Ukraine meets nearly all biological, climatic, and environmental‑health criteria relevant to the Winter PK Matrix and the Geo‑Resilience Compass. The country exhibits pronounced continental winters, strong seasonal infection patterns, significant environmental burdens, and large geographical gradients — a combination that makes it a highly compelling model environment for seasonal biology, PK shifts, and resilience mechanisms. Winter extremes and seasonality: Ukraine experiences long, cold winters with extended periods of darkness, dry air, and marked peaks in respiratory infections (influenza, RSV, adenoviruses, bacterial pneumonias). These factors strain barrier integrity, modulate immune axes, alter microbiome profiles, and may promote seasonal pharmacokinetic shifts. As a result, the 8‑axis (barrier–infection–microbiome) is particularly active here. Environmental stress and AHR axes: Urbanized regions such as Kyiv, Dnipro, Kharkiv, and Odesa show significant exposures to PM2.5, industrial emissions, coal and biomass combustion, and winter inversion events. These stressors activate AHR‑ and NRF2‑dependent signaling pathways, influence transporter expression (e.g., SLC and ABC transporters), and modulate inflammatory and metabolic axes — a central mechanism underlying PK variability. Climatic and geographical range:
Ukraine spans multiple climate zones — from continental winter regions to milder Black Sea areas. This allows seasonal patterns, PK shifts, and barrier stressors to be examined on a zone‑specific basis, making the country an ideal test field for the Winter PK Matrix. Infection patterns and seasonal dynamics: Recurring annual infection waves (RSV, influenza, bacterial respiratory infections) as well as seasonal declines in vitamin D levels indicate strong activation of the 17‑axis (AHR/Th17/TBX21) and the 8‑axis. These patterns are biologically highly relevant and may explain clinically meaningful PK shifts. Relevance for the Geo‑Resilience Compass: The combination of climatic seasonality, environmental stress, urban exposure, demographic challenges, and a heterogeneous healthcare infrastructure makes Ukraine an ideal application case for the Geo‑Resilience Compass. The country provides an environment in which environmental stress, immunomodulation, barrier biology, and pharmacokinetic dynamics interact in particularly clear and pronounced ways.
6. United States: The United States is characterized by an exceptionally high degree of climatic diversity — ranging from arctic, continental, and temperate zones to subtropical and desert regions. This allows the Winter PK Matrix to be applied in nearly all climatic contexts, making the U.S. an ideal test field for cross‑zone model validation. In urban areas, substantial environmental burdens arise from PM2.5, NOx, ozone, and traffic‑related emissions. These factors render the AHR‑dependent environmental and inflammatory axes biologically highly relevant and influence transporter expression, barrier integrity, and inflammatory signaling pathways. At the same time, the U.S. is among the global leaders in pharmacokinetics, immunology, AHR research, microbiome sciences, and systems biology. The availability of large, high‑resolution health and research datasets (e.g., from integrated health systems, cohort studies, and biomedical databases) makes the country an ideal integration environment for the Geo Resilience Compass. The high prevalence of chronic diseases — including metabolic syndromes, cardiovascular diseases, COPD, and inflammatory disorders — further amplifies the relevance of the 17‑axis, as barrier dysfunction, chronic inflammation, and immunological aging processes substantially modulate seasonal biology and pharmacokinetic profiles.
Thus, the United States functions as a global multiplier for the Winter PK Matrix: a country in which climatic diversity, environmental stress, chronic disease burden, and excellent data availability converge in a uniquely powerful way.
7. India: In India, the winter period largely coincides with the pronounced smog season, which is characterized by extreme PM2.5 burdens, industrial emissions, biomass burning, and traffic aerosols. This constellation leads to strong activation of AHR‑dependent environmental and inflammatory axes and makes India one of the globally most relevant AHR hotspots. In parallel, India exhibits a high seasonal infection burden, including RSV, influenza, bacterial respiratory infections, pneumonias, as well as enteric and vector‑borne diseases. The combination of high population density, urban exposure, regional mobility, and climatic heterogeneity results in significant strain on the barrier, microbiome, transporter, and immune axes — the 8‑axis is particularly dynamic here. India encompasses tropical, subtropical, and temperate climate zones within a single country and therefore displays an exceptional range of seasonal biological patterns. This climatic and demographic diversity makes India a biologically highly relevant model environment for the Winter PK Matrix and the Geo Resilience Compass.
8. China: China encompasses arctic–subarctic zones (Heilongjiang, Jilin), continental winter regions (Beijing, Tianjin, Hebei), subtropical zones (Shanghai, Jiangsu, Zhejiang), and tropical regions (Hainan, southern Guangdong) → the Winter PK Matrix could be tested across all climatic modes. China shows massive annual peaks in influenza, RSV, adenoviruses, bacterial respiratory infections, enteric infections, and vector‑borne diseases in the south → barrier, microbiome, transporter, and immune axes may be strongly modulated seasonally. China also experiences substantial environmental burdens from PM2.5, ozone, industrial emissions, coal combustion, traffic, and winter smog episodes → AHR‑ and NRF2‑dependent axes are biologically extremely relevant. Urbanization + population density → strong barrier and infection stress. Megacities such as Beijing, Shanghai, Guangzhou, Shenzhen, and Chongqing create an environment in which barriers may be continuously challenged, infection pressure is high, and transporter expression may be dynamically modulated → a perfect urban stress test, similar to Hong Kong but on a much larger scale. Hong Kong: Hong Kong exhibits a tropical–subtropical climate profile that can be associated with high infection pressure and clearly defined seasonal patterns. The region is also among the urban areas with high air pollution levels in East Asia — particularly due to PM2.5, ozone, and traffic‑related emissions. These exposures make the AHR‑dependent environmental and inflammatory axes biologically highly relevant. The high population density leads to intensive use of shared indoor spaces and thus to significant strain on the barrier and infection axes. At the same time, Hong Kong possesses excellent health data. This could make Hong Kong an ideal urban “stress test” for the Winter PK Matrix and the Geo Resilience Compass — an environment in which barrier integrity, microbiome dynamics, infection pressure, and environmentally induced AHR modulation interact in particularly pronounced ways.
9. The United Kingdom: The United Kingdom clearly belongs on the “core list” for me. Especially in urban centers such as London, Birmingham, Manchester, and Glasgow, PM2.5, NOx, traffic emissions, and heating exhaust are relevant exposure factors. This means that the AHR axis may be markedly activated on a seasonal basis, transporters such as ABCB1 and SLC22 may be modulated, and PK shifts appear plausible. The UK would also be an ideal test field for the Geo Resilience Compass: as an island state with clear environmental boundaries, a mix of urban and rural areas, strong governance structures, high technological maturity, and excellent data availability, it functions as a genuine “resilience laboratory.” In addition, an aging population makes the 17‑axis particularly relevant: aging societies exhibit barrier dysfunction, immunosenescence, and increased susceptibility to infections. The UK therefore forms an ideal contrast to younger countries such as Pakistan and significantly expands the scope of the Winter PK Matrix.
10. South Africa: South Africa exhibits a clearly defined seasonal biology: the winter period corresponds to the dry season and is associated with pronounced peaks in respiratory infections, while the summer months are shaped by the rainy season and a shifted pathogenic spectrum. Seasonal fluctuations in UV exposure suggest relevant modulation of the vitamin D axis, and the dry winter air leads to increased stress on epithelial barriers. South Africa therefore displays a clearly delineable, biologically modellable “winter effect.” Epidemiologically, this is relevant for RSV, influenza, tuberculosis, HIV‑associated immunomodulation, bacterial respiratory infections, and pneumonias during the dry season. This constellation implies a pronounced seasonal activation of the 8‑axis (barrier, microbiome, infection, transporters, immune response). In parallel, environmental burdens in urban centers are substantial: elevated PM2.5 concentrations, biomass burning, industrial emissions, and seasonal air pollution activate AHR‑ and NRF2‑dependent stress and detoxification axes. These axes, in turn, modulate transporter expression, barrier integrity, and inflammatory signaling pathways and are therefore highly relevant for pharmacokinetic and immunological seasonality. Added to this is pronounced climatic diversity — Mediterranean, subtropical, semi‑arid, and high‑altitude climate zones — which makes South Africa an ideal model environment for investigating climate‑zone‑specific and trans‑zonal resilience mechanisms.
11. Africa: other highly relevant countries: Kenya, Egypt, Nigeria, and others
12. Pakistan: Pakistan would also be a key country for the Winter PK Matrix, as it unites tropical, subtropical, and temperate climate zones within a single nation. This makes Pakistan a biologically highly compelling case for my model — the winter biology is clearly pronounced here. In its relevance, Pakistan is in no way inferior to countries such as India and China. For me, it represents an ideal “8‑axis case.” A young population implies higher transmission: children in schools generate strong transmission dynamics, young adults are highly mobile, close household structures increase contact intensity, and lower social isolation leads to more interaction. At the same time, there is substantial exposure to environmental stressors such as traffic, smog, and urban density. All of this can lead to an elevated baseline activity of the 8‑axis: barriers are stressed more frequently, microbiomes are more strongly disrupted, and transporters as well as PK profiles may exhibit more pronounced seasonal changes.
13. Australia: Australia exhibits extreme seasonal fluctuations in UV exposure, which strongly modulate the vitamin D axis and contribute to distinct seasonal biological patterns. The country spans both tropical and temperate climate zones, allowing the coexistence of two fundamentally different climatic modes within a single national framework. This dual‑mode climate architecture makes Australia a uniquely valuable model environment for the Winter PK Matrix, as both tropical and temperate seasonal dynamics — including barrier stress, immune modulation, microbiome shifts, and potential PK variability — can be studied in parallel.
14. Brazil: Brazil exhibits a pronounced seasonal biology that can certainly be clearly modeled despite its tropical and subtropical climate zones. The winter period corresponds to the dry season in many regions and is associated with distinct peaks in respiratory infections, while the rainy season produces a shifted pathogenic spectrum. This dynamic makes Brazil a biologically highly relevant case for the Winter PK Matrix. Tropical + subtropical + temperate → multiple climate modes in one country, i.e., Brazil encompasses Amazonian tropics, subtropical southern regions, and temperate highland zones. This could potentially allow different seasonal patterns to be examined in parallel — an ideal multi‑zone test case. Seasonal infection patterns: Brazil also shows clear peaks in influenza, RSV, adenoviruses, bacterial respiratory infections, dengue, Zika, and chikungunya (vector‑borne, rainy‑season dependent) → The 8‑axis (barrier–infection–microbiome–transporter) is strongly seasonally active. Environmental stress and AHR axes: In urban centers such as São Paulo, Rio de Janeiro, Belo Horizonte, and Porto Alegre, there are relevant exposures to PM2.5, ozone, industrial emissions, traffic, and biomass burning → AHR and NRF2 axes are strongly activated, modulating transporter expression, barrier integrity, and inflammatory signaling pathways.
UV and vitamin D dynamics: Despite tropical latitudes, many regions may show seasonal UV fluctuations that influence the vitamin D axis — particularly in the south. Demographics and urbanization: Brazil has a young, highly mobile population, extreme levels of urbanization, dense household structures, and high infection dynamics → A perfect “8‑axis case.”
Relevance for the Geo Resilience Compass: Brazil is a country in which climatic diversity, environmental stress, infection pressure, social heterogeneity, urban density, and regional inequality interact in particularly complex ways. This makes it an ideal environment for analyzing resilience mechanisms, seasonal PK shifts, and environment–biology couplings.
15. France: An underestimated high‑risk candidate for environmental and barrier axes. 1. High pesticide stress → AHR, PXR, CAR and NRF2 axes highly relevant. France is among the European countries with very high agricultural intensity, large‑scale pesticide use (herbicides, fungicides, insecticides), and significant exposure in rural and peri‑urban areas → the AHR axis, as well as PXR/CAR detoxification axes, could be strongly activated. → This modulates transporters (ABCB1, ABCCs, SLCs), barrier integrity, and inflammatory signaling pathways. Strong seasonality in temperate zones - France has clear winter–summer contrasts: Winter: infection peaks (influenza, RSV, bacterial respiratory infections) / Summer: ozone burden, heat, UV fluctuations → The 8‑axis (barrier–infection–microbiome–transporter–immune response) is well modelable seasonally. Urban environmental stress in cities such as Paris, Lyon, Marseille, and Lille, i.e., they show relevant burdens from PM2.5, NOx, ozone, traffic, and heating emissions → AHR axis + barrier axes are additionally stressed. 4. Agriculture + urbanization → double stress. France is one of the few countries where intensive agriculture (pesticides, ammonia, particulate matter) and dense urban areas (traffic, industry, ozone) coexist in close proximity → This creates complex exposure patterns, ideal for your model. 5. Excellent data availability - France has strong epidemiological cohorts (e.g., CONSTANCES), good health data, and high research density in toxicology, immunology, and microbiome science → Very well suited for the Geo Resilience Compass.